HLA plays an important role in the immune system and is more and more leveraged in HLA-restricted precision medicine therapies, as shown by the increasing number of HLA-restricted therapies in the clinic (check our blog post “The role of HLA in immunotherapy development”). Understanding the different and sometimes contrasting roles of HLA in healthy tissue and during tumor progression is important to further comprehend how HLA may be leveraged in therapy development strategies. Novel therapies may, for example, exploit HLA diversity and expression patterns to specifically target cancer cells or be developed to bind emerging targets. Additionally, HLA typing of patients may be used to determine which patients are eligible for HLA-restricted therapies. Finally, patients’ HLA genotype may explain why some patients fail to respond to immune checkpoint inhibitors.
We are launching a new blog post series to further explore the role of HLA in the tumor microenvironment. Throughout this series, we will first introduce several key players of the HLA system in their healthy physiological context and their role in the tumor microenvironment. We will then dive into how cancer may modulate the HLA system to evade immune detection. Finally, we will explore the implications for immunotherapy, including how HLA status and genetic variation may serve as predictors of therapeutic response.
Stay tuned for the upcoming posts in this series!
Role of HLA under healthy conditions
HLA molecules involved in immune activation are broadly divided into two classes depending on their roles in antigen presentation. Under normal physiological conditions, HLA Class I molecules (HLA-A, -B, and -C) act as a surveillance display system on the surface of virtually all nucleated cells, continuously presenting peptide fragments (antigens) derived from intracellular protein turnover.
These peptides are generated by proteasomal degradation of cytosolic proteins and transported into the endoplasmic reticulum (ER), where they are loaded onto HLA Class I molecules (see figure below). Specific adaptive immune cells (CD8+ cytotoxic T cells) respond to peptides that are presented by HLA Class I molecules through their T-cell receptors (TCR). In this way, under healthy conditions, self-peptides (when expressed at normal levels) are generally ignored due to immune tolerance mechanisms. The same mechanism triggers T cell activation and targeted cell killing when non-self peptides are recognized, derived for example, from intracellular pathogens, aberrantly expressed or mutated cancer proteins [1].
On the other hand, HLA Class II molecules (including HLA-DP, -DQ, and -DR molecules) are primarily expressed on Antigen Presenting Cells (APCs), such as dendritic cells, macrophages, and B cells. APCs are capable of internalizing foreign particles or cellular debris, processing it and presenting the resulting antigens on HLA Class II molecules (see figure below). These antigens presented by HLA Class II may then be recognized by the TCR on a CD4+ T cell, which (together with co-stimulatory signals) initiates an immune response. APCs drive CD4+ helper T cell responses, which are critical in modulating the magnitude and durability of cytotoxic responses through cytokine secretion. These helper T cells support B cell antibody production, and may influence the efficacy of cancer immunotherapies. Internalized proteins are degraded in endosomal/lysosomal compartments, where peptides are loaded onto HLA Class II molecules (see figure below). CD4+ T cells are important immunomodulators that aid the activity of other immune cells by releasing cytokines [2].
A clinically relevant subset of non-classical HLA Class I molecules, particularly HLA-E and HLA-G, has been described to have inhibitory effects on immune responses. HLA-E interacts with both activating and inhibitory receptors on Natural Killer (NK) cells, helping to fine-tune immune activity. HLA-G, on the other hand, is best known for its role during pregnancy, where it contributes to immune tolerance in the maternal-foetal interface. While HLA-E is expressed at low levels in most tissues, HLA-G expression is more restricted, primarily to placental trophoblasts present during pregnancy. Critically, both molecules are aberrantly overexpressed in various cancers, where they serve as immune checkpoints that help tumors evade destruction — a mechanism with direct therapeutic implications that will be discussed in the upcoming blog post in this series [3, 4].
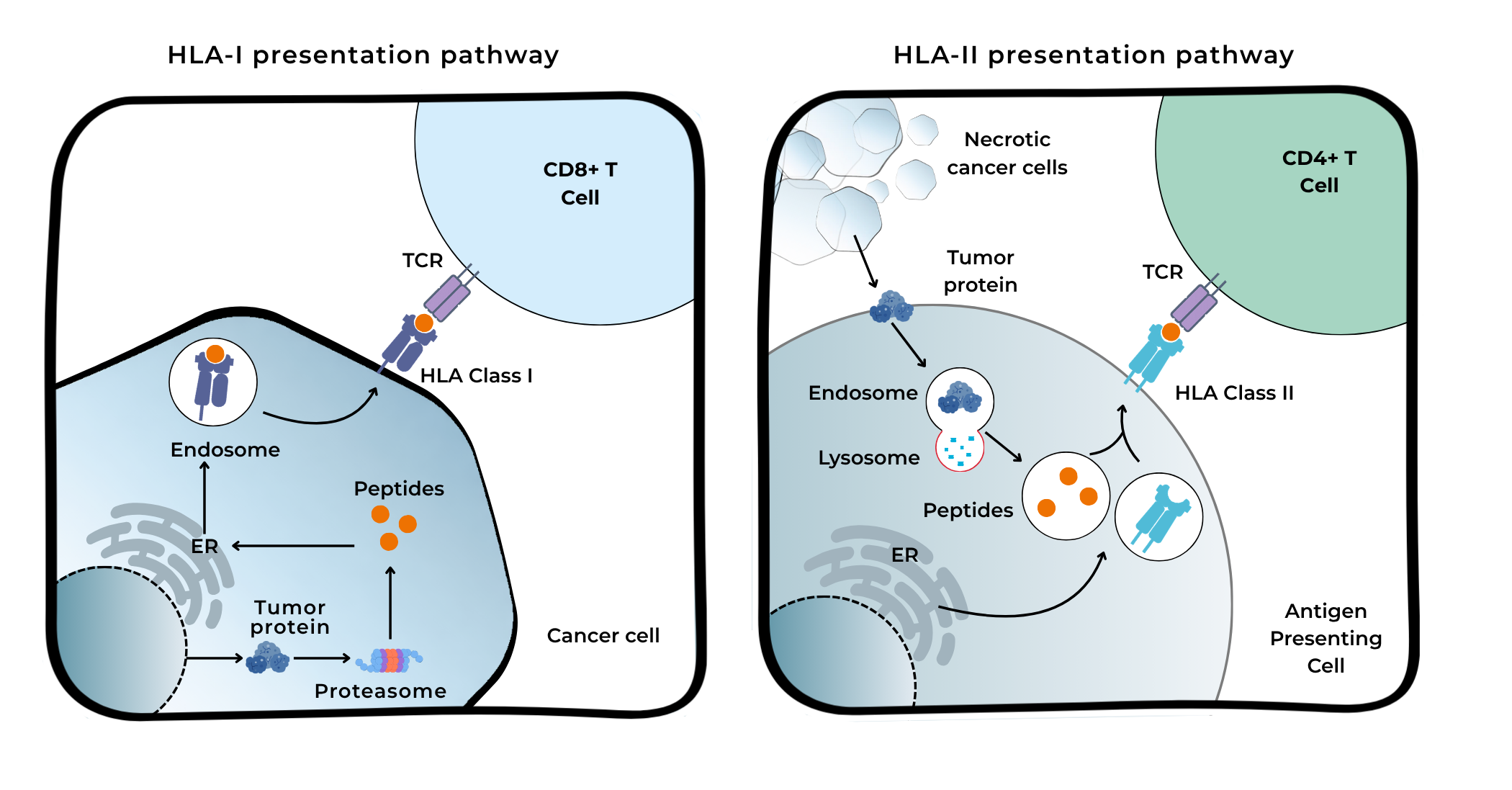
Figure: HLA-I and HLA-II antigen presentation pathways
Role of HLA in the tumor microenvironment
HLA molecules are central to shaping the immune landscape within the tumor microenvironment. Tumors can exploit multiple layers of HLA biology to evade immune detection, with direct implications for therapeutic response. Loss or downregulation of HLA Class I is an established mechanism of primary and acquired resistance to T cell-directed immunotherapies, including PD-1/PD-L1 checkpoint inhibitors. When antigen presentation via HLA Class I is reduced, CD8+ T cell recognition of cancer cells is severely impaired, limiting the effectiveness of checkpoint blockades. This underscores why the assessment of HLA Class I expression in tumor biopsies may become increasingly relevant in precision oncology [5].
Beyond resistance mechanisms, HLA biology within the tumor microenvironment is a key determinant of immunotherapy efficacy. Firstly, the HLA genotype is emerging as a predictor of immunotherapy response, though this remains an evolving area of research. Secondly, HLA-restricted therapies are explicitly designed to exploit specific HLA alleles to drive targeted immune killing of tumor cells. However, tumor-driven HLA alterations (including HLA Class I downregulation and overexpression of non-classical molecules like HLA-E and HLA-G) may limit the efficacy of these strategies [3]. Understanding this interplay of HLA molecules between therapeutic design and tumor immune escape will be essential as HLA-restricted therapies move through clinical development.
In the upcoming blog post, we will further explore how tumors evade the immune system by impairing HLA molecules. To stay informed about future posts in this series, check our website regularly for upcoming updates and new articles.
Authors:
Stephanie Ahrendt – Global Medical Scientific Liaison Manager
 Stephanie has a strong background in molecular biology and genetics, and has extensive experience across oncology, endocrinology, and nuclear medicine. In her current role at Eurobio Scientific, she is dedicated to advancing innovative therapies and fostering collaboration between science and clinical practice.
Stephanie has a strong background in molecular biology and genetics, and has extensive experience across oncology, endocrinology, and nuclear medicine. In her current role at Eurobio Scientific, she is dedicated to advancing innovative therapies and fostering collaboration between science and clinical practice.
Valentina Manzini – Project Coordinator CDx

Valentina holds a PhD in Molecular Biology, with a background in tumor biology. She is currently working at GenDx, supporting the Companion Diagnostics team by ensuring projects run smoothly, performing regulatory submissions and coordinating IVD activities of clinical trials involving both drugs and CDx.
References:
[1] Abbas, A. K., Lichtman, A. H., & Pillai, S. (2021). Cellular and molecular immunology (10th ed.). Elsevier.
[2] Zhu, X., & Zhu, J. (2020). CD4 T helper cell subsets and related human immunological disorders. International Journal of Molecular Sciences, 21(21), 8011.
[3] Benitez Fuentes, J. D., Bartolome Arcilla, J., Mohamed Mohamed, K., Lopez de Sa, A., de Luna Aguilar, A., Guevara-Hoyer, K., … & Sánchez-Ramon, S. (2024). Targeting of non-classical human leukocyte antigens as novel therapeutic strategies in cancer. Cancers, 16(2), 421.
[4] Fisher, J. G., Doyle, A. D. P., Graham, L. V., Khakoo, S. I., & Blunt, M. D. (2022). Disruption of the NKG2A:HLA-E immune checkpoint axis to enhance NK cell activation against cancer. Clinical & Experimental Immunology, 209(2), 107–116.
[5] McGranahan, N., Rosenthal, R., Hiley, C. T., Rowan, A. J., Watkins, T. B. K., Wilson, G. A., … & Swanton, C. (2017). Allele-specific HLA loss and immune escape in lung cancer evolution. Cell, 171(6), 1259–1271.e11.